I’ve always heard doctors and professors alike refer to the human body as “a major engineering feat of nature” – but I never quite believed them with conviction until this very week. Don’t get me wrong, I have always appreciated that the human body was a complex network of dynamic biological and physical interactions…but (being the engineer that I am) I never thought much more than that. Today, and perhaps for a long time hereafter, I think it’s safe to say that I now see the human body as a source of inspiring efficiency and elegance that we researchers and engineers have yet to surpass.
The pivotal surgery that I observed this week was an aortic valve replacement surgery, perhaps one of the most invasive and risky ones I’ve seen yet! More specifically, the procedure involved an ascending aneurism repair that used a valve-sparing protocol through which a synthetic Dacron aortic graft (one which is inert and will eventually allow the body to grow a new lining of cells around it) was sewn in to replace part of a patient’s damaged/weakened ascending aorta. This was my first time seeing a live, beating heart in a chest – and, to be honest, it was an epic sight! (To see a beating heart is much more compelling than understanding the “idea” of a beating heart, by far) To think that human tissue can physically beat on its own, to its own innately defined rhythm, is truly a biological engineering feat to be respected.
This surgery was saddening in that the patient was a 25 year old girl who, in all cases but one, was in perfect health. She was fit and healthy, and she neither smoked nor exposed herself to hazardous health situations. Ultimately, the main source of her landing in the OR at such an early age was beyond her control and beyond anyone’s expectations – it was the fact that she had developed Loeys-Dietz syndrome, a recently-discovered autosomal dominant genetic syndrome which is similar to Marfan syndrome. The main difference is that the Loeys-Dietz syndrome is caused by mutations in the genes encoding transforming growth factor beta receptor 1 (TGFBR1) or 2 (TGFBR2). Because of these mutations, these patients are prone to serious heart complications, such as aneurisms. In this case the girl had an ascending aneurism, (roughly) meaning that there was an abnormal bulge in the wall of the aorta. The aneurysm occurred at the aortic root, causing the aorta to dilate or widen and the aortic valve to leak. Without treatment the girl would have definitely developed a life-threatening condition called aneurysm dissection – essentially, blood would flow through a tear in the inner layer of the aorta, causing the layers to separate, and eventually blood flows would induce the arterial wall to burst. (After which a lot of bad things happen all too quickly).
The procedure used on this 25-year old girl was called the Modified David’s Reimplantation Procedure, which is basically a valve-sparing aortic root replacement surgical treatment for aortic root aneurysms. Via this method, the aneurysm is repaired while the patient's own aortic valve is preserved to the best of the surgeon’s ability. (I think they use the word “preserved” loosely here, as to sew the remaining aortic valve to the valve graft they had to split the aortic valve along its sides and open it up in leaflet like strips such that the whole thing looked like a blossoming flower with star-like petals prior to graft attachment). I will admit that it looked very cool, but I felt bad for the patient whose valve was getting all sliced up. Some pros to this procedure are: the method helps avoid the use of long-term anticoagulant (blood-thinner) medications, and it may reduce the risk of stroke or endocarditis. I am not sure how truly “sparing” the procedure is, since this girl’s aortic valve could not be used fully (it was shorter than normal) and thus a bioprosthetic valve graft was added to her heart.
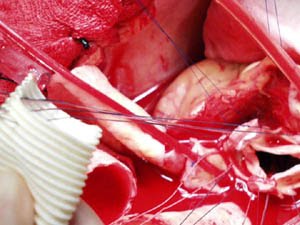
After talking to the surgeons and nurses I was able to gather enough medical terms to research the procedure that I just observed. From the Cleveland Clinic website (http://my.clevelandclinic.org/default.aspx) I was able to get the following images, which are pretty similar to what I witnessed with my own eyes in the Cornell OR.
1) Photograph of aortic valve prior to tube graft addition to aortic root

2) Photograph of Dacron aortic graft prior to insertion

3) Sutures are sewn through the annulus of the aortic valve and the bottom portion of the Dacron graft
4) The graft is being lowered into place, around the outside of the aortic valve.

5) If you peer inside the graft (top view), you can see the aortic valve. The aortic valve is secured within the new tube and the coronary arteries are reattached. The other portion of the graft is then sewn to the aorta.

In the interest of time and blog-space, I will cut the rest of my thoughts a little short – but rest assured I was very impressed by the whole procedure and the army of nurses and technicians at the scene! I don’t think I mentioned it yet, but there was also a machine with a ton of tubes and pumps that was used to circulate the girl’s blood while her heart was being operated on. I am pretty sure they had to stop (or slow down severely?) her heart so it stayed still for the procedure, which lasted about 5 hours. Her body had to be chilled and after the graft was in place the surgical bed had to be tilted at a near-40 degree angle (with her head on the lowered end) so that warm blood could rush through and fill up her heart more quickly. The whole operation was an amazing feat of sewing, cutting, tissue maneuvering, and timing – but if the patient had seen what I had seen I am not sure if she would go through with it. Is this a case of “ignorance is bliss”? What few of us realize is how much trust patients put in their doctors and in the medical devices that doctors use. I hope that one day surgeries like this will be less invasive and strenuous on the body, because patients like this girl have so much life to live but they may be held back by procedures like this which can severely their hearts.
Summer Immersion Project: Review/analysis of dermal fillers and hydrogel grafts
After much reading and discussion with my mentor Dr. Grant, I have finally settled on a project! It took me a bit longer than I thought because I was trying to find a project that made some connections between what I’ve observed and learned about in the clinic with what I test and investigate in the lab. Overall my project will focus on a review/analysis of the full spectrum of dermal fillers and injectable gels (i.e. those made from microparticles, Hyaluronic acid, bovine and human collagen, etc.) from an engineering viewpoint, with the goal of defining key problems, trends, and techniques and offering insight into future endeavors. I hope to bring in another angle to the discussion – one from the pure lab-bench perspective. I am currently part of a lab that pioneers novel biomaterials made entirely of synthetic strands of DNA. We have recently developed a hydrogel made of multiple-linked double stranded DNA that, in the presence of cell lysate and other protein-forming materials, can produce a high yield of proteins in a cell-free context. Up to this point I have only thought of and analyzed hydrogels and biomaterials from a pure science view, but now I plan to integrate my pure science background with my new clinical observations. I have already watched Dr. Grant employ different dermal fillers for face augmentation and wrinkle minimization in older patients, in addition to starting to research relevant articles for deepening my understanding of the clinical applications and complications of dermal fillers. In the week to come I will collect information from these articles and my observations with Dr. Grant and start to delineate an outline for my analysis and synthesis of what I have found.
No comments:
Post a Comment